#page 3253
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr.com is the 103rd most visited website in the world.
Text
Karkat Vantas, Jade Harley
Act 5, page 3250-3253
-- carcinoGeneticist [CG] began trolling gardenGnostic [GG] --
CG: ATTENTION HARLEY.
CG: PLEASE STOP WEEPING WITH AND OR BEATING THE SHIT OUT OF YOUR SELF PROTOTYPED LUSUSPRITE
CG: STOP DOING ONE OF THOSE THINGS AT LEAST
CG: LONG ENOUGH TO ANSWER ME.
CG: PLEASE.
CG: PRETTY POLITE EARTH PLEASE.
CG: WHO AM I KIDDING
CG: I'M WASTING MY TIME AGAIN
GG: karkat!!!!!
CG: WHOA FUCK
CG: YOU ANSWERED ME, I DONT BELIEVE IT
GG: yes
GG: im going crazy here
GG: i never thought id say this, but im actually almost relieved to talk to you
CG: WHAT
CG: YOU ARE
GG: or really ANYBODY besides that lunatic
GG: SHE IS DRIVING ME NUTS!!!!!!!
CG: OH YEAH?
CG: HOW SO, EVERYTHING HERE APPEARS TO BE PROCEEDING RATIONALLY.
CG: WHAT SEEMS TO BE THE PROBLEM
GG: are you joking??? look at this mess!
CG: MESS? JADE, NOW IT SOUNDS TO ME LIKE *YOU'RE* THE ONE WHO'S JOKING.
CG: YOUR HIVE BALL ROLLED DOWN A BEAUTIFUL WINTER HILL, AND YOU ARE SPENDING SOME QUALITY TIME WITH FAMILY.
CG: YOU ARE GOING TO HAVE TO FILL ME IN ON THE NATURE OF THE PROBLEM.
GG: okay...
GG: i made the mistake of prototyping my dream self who has been dead for years
GG: and shes completely crazy and theres no talking any sense into her
CG: HMM.
GG: hmm?
CG: YES. "HMM."
GG: hmm what
CG: HMM AS IN HMM INTERESTING.
CG: AS IN HMM HOW VERY, VERY FUCKING INTERESTING INDEED.
GG: :\
GG: what are you getting at???
CG: WHAT DO YOU MEAN WHAT AM I GETTING AT.
CG: I'M GETTING AT WHATEVER HMM INTERESTING GETS AT.
CG: PLEASE GO ON, I'M LISTENING TO YOUR PROBLEM.
GG: well...
GG: i mean, i understand why she is upset
GG: but she is completely inconsolable, and wont listen to reason about anything!
GG: and i guess i could deal with that but...
GG: the frustrating thing is that shes actually me :(
GG: i really dont think i would act like that
CG: HMMMMM.
GG: will you stop saying hmm!!!!!!
CG: OK, FINE.
CG: WHAT OTHER SEQUENCE OF LETTERS WOULD YOU HAVE ME USE TO REGISTER MY PROFOUND FASCINATION.
GG: fascination?
GG: what do you find so fascinating?
CG: I'M JUST TRYING TO UNDERSTAND.
CG: I AM BEING SENSITIVE ABOUT IT INSTEAD OF A RAGING FUCKASS, ISN'T THAT WHAT YOU WANT.
CG: YES, IT IS, IF YOU DON'T BELIEVE ME JUST ASK FUTURE YOU, ASSUMING THAT CONVERSATION DOESN'T MAKE YOU CRY AS WELL.
CG: NOW TELL ME MORE ABOUT YOUR FEELINGS.
GG: my feelings?
CG: YES, HOW DID THIS MAKE YOU FEEL.
GG: well...
GG: at first i was sad
GG: because she made me remember all the sad things that just happened
GG: but im trying to be strong about all that so we can keep moving forward
GG: and if i can then why cant she?
GG: but she just went on and on
GG: and i started getting angry...
GG: ugh i have never been so angry in my LIFE!!!
CG: HMMMMMMMMMMMMMMMMMMMMM.
GG: I SAID STOP SAYING FUCKING HMM
CG: o:B
GG: what does THAT mean?????
GG: is that supposed to be someone with a halo and goofy teeth?
GG: ARE YOU MAKING FUN OF ME?
CG: NO, NO
CG: YOU'RE LOOKING AT IT BACKWARDS
CG: THOSE ARE MY HORNS
GG: oh
GG: haha oops
CG: OK SO IF I'M UNDERSTANDING YOU
CG: YOU'RE ANGRY AT A VERSION OF YOURSELF FROM A DIFFERENT POINT IN TIME
CG: BECAUSE SHE'S BEING AN OVERLY EMOTIONAL SHITHEAD WHO IS BASICALLY THE MOST REVOLTING SELF LOATHING PIECE OF FILTH YOU HAVE EVER MET
CG: AM I FOLLOWING
GG: yeah, pretty much
CG: I'M NOT GOING TO SAY HMM AGAIN
CG: BUT COME ON
CG: DON'T YOU FIND THE SITUATION TO BE JUST THE SLIGHTEST BIT INTERESTING?
CG: I MEAN, CONSIDERING
GG: considering what??
CG: IF I RECALL, IT WASN'T THAT LONG AGO FROM EITHER OF OUR PERSPECTIVES THAT YOU WERE RIPPING ON ME AND MY SMUG WINDBAG FUTURE SELF FOR ARGUING WITH EACH OTHER
GG: oh come on...
GG: this is NOTHING like that!
CG: HOW IS THIS NOT LIKE THAT
GG: because she's...
GG: well
GG: she's ACTUALLY INSANE
CG: OH I SEE, AND ALL THOSE IDIOT PAST AND FUTURE KARKATS WEREN'T???
GG: but
GG: those are you
GG: im not her!
CG: OH AREN'T YOU
CG: YOU JUST SAID YOU WERE, I JUST HEARD YOU SAY THAT
CG: SO TELL ME
CG: HOW IS THIS EVEN THE SLIGHTEST FUCKING BIT DIFFERENT?
GG: i dont know
GG: it just...
CG: YES, GO ON
CG: I'M REALLY CURIOUS
CG: HOW
GG: ...
GG: oh my god
GG: youre right :(
GG: so then i guess
GG: im a hypocrite :(
CG: NOT REALLY
CG: IT JUST MEANS YOU'RE A SANE RATIONAL PERSON, AND THERE JUST MIGHT BE HOPE FOR YOU YET
GG: wait...
GG: so me arguing with my dead dream self
GG: and smacking her around while screaming at her
GG: makes me SANE???
CG: YES, ABSOLUTELY.
CG: IT MEANS ALL OF YOUR HIDEOUS FLAWS DISGUST YOU.
CG: YOU ARE RIGHT TO BE DISGUSTED, IT'S MORE THAN MOST PEOPLE CAN SAY FOR THEMSELVES.
CG: REALLY, CONGRATULATIONS ARE IN ORDER.
GG: hahaha, wow
GG: you are so weird
CG: CONGRATULATIONS, IN ADDITION TO, JUST MAYBE, AN APOLOGY.
CG: DON'T YOU THINK?
GG: you want me to apologize?!
GG: for what, calling you crazy for arguing with yourself???
CG: WOULD IT REALLY KILL YOU TO CONSIDER IT?
GG: after taking so much crap from you for all those years?
GG: no forget it, im not apologizing that is BULLSHIT
CG: DEAD DREAM DOG JADE, IS THAT YOU??? YOU'RE SOUNDING A BIT HYSTERICAL, MAYBE YOU SHOULD CALM DOWN.
GG: shut uuuup!!!
CG: WELL IF YOU CAN MANAGE TO GET YOUR ANEURYSM UNDER CONTROL
CG: MAYBE YOU WILL REALIZE I DIDN'T ACTUALLY SPECIFY TO WHOM AN APOLOGY WAS IN ORDER.
CG: IDIOT.
GG: what
GG: are you saying you want to apologize
CG: I GUESS
CG: THIS APOLOGY WAS GOING TO GO DOWN ONE WAY OR ANOTHER, SO THIS MIGHT AS WELL BE THE TIME.
CG: AND LET'S FACE IT, I WAS REALLY BEING THE WORST KIND OF PHLEGM BUBBLE BLOWN OUT A NOISY GLISTENING ASS.
CG: SO I'M SORRY.
CG: BUT TO BE FAIR, IT WAS MY PAST SELF WHO WAS GIVING YOU SUCH A HARD TIME, AND HE'S COMPLETELY DERANGED.
GG: ok, i appreciate the THOUGHT of an apology, but i dont know if it really counts if you are just going to pawn off responsibility on your "past self" again!
GG: maybe your "present self" should own up to it!
CG: YEAH THAT'S WHAT HE'S DOING.
CG: HE, BEING ME, RIGHT NOW, IS OWNING UP TO WHAT A FUCKING RETARD PAST ME WAS, AND CONTINUES TO BE.
GG: laaaaame
CG: YES, I KNOW IT'S LAME.
CG: OR I KNOW THAT YOU THINK IT'S LAME WHEN I SAY SHIT LIKE THAT.
CG: BECAUSE REMEMBER
CG: I HAVE BEEN TALKING TO YOU FROM THE FUTURE, AND I KNOW YOU DON'T COTTON TO MY PCG/FCG STUPIDITY.
CG: BUT SEE, YOU DON'T KNOW THAT YOU KNOW THAT YET.
CG: OR MORE SPECIFICALLY, YOU DON'T KNOW THAT I KNOW THAT YOU KNOW THAT YET.
CG: SO I'M KIND OF PULLING A FAST ONE HERE.
GG: hahahaha, that is so ridiculous
GG: why dont you stop it with all this nonsense and own up to being terrible unequivocally?
CG: YEAH I'M GOING TO.
CG: THE THING IS, I KIND OF MISREPRESENTED MYSELF.
CG: I'M NOT AS MUCH OF A SCUMBAG AS I WAS SO DETERMINED TO MAKE OUT WITH MYSELF TO BE.
CG: FUCK I MEAN
CG: MAKE MYSELF OUT TO BE
GG: :o
CG: I REALLY DON'T KNOW WHY I TROLLED YOU LIKE THAT SO PERSISTENTLY
CG: FOR SOME REASON DEEP DOWN I JUST KNEW THAT I HAD TO
CG: EVEN IF IT MEANT DIGGING MYSELF INTO A HUGE HOLE WITH YOU AND EVERYONE ELSE THAT WOULD BE HARD TO CLIMB OUT OF
CG: AND LIKE PRACTICALLY EVERYTHING I SAID WAS COMPLETELY BASELESS BECAUSE I DIDN'T ACTUALLY KNOW YOU
CG: JUST LIKE YOU DIDN'T AND STILL DON'T ACTUALLY KNOW ME
CG: SO I GUESS I AM APOLOGIZING FOR IT, LIKE REALLY SERIOUSLY NOW.
CG: I, PRESENT KARKAT, IN THE CURRENT MOMENT, APOLOGIZE ON BEHALF OF MY STUPID PAST SELF, *WHO IS ACTUALLY ME*.
CG: THE GUY TALKING RIGHT NOW.
CG: LIKE, THERE'S NO DIFFERENCE BETWEEN THOSE GUYS, OK?
GG: hmmmm...
CG: HMMMM???????
GG: yes, hm
CG: HM WHAT
GG: ok karkat, that sounds pretty sincere to me
GG: and youre right, i dont actually know you
GG: i just know the part of you who acted like a bully
GG: i understand there can be more to a person than just the stuff they say when theyre angry
GG: so i will accept your apology and give you another chance
CG: OK, GREAT.
GG: and i will apologize for calling you crazy
GG: obviously i am not in much position to judge :|
CG: NO BUT
CG: YOU WERE RIGHT, I AM CRAZY
CG: BUT THANKS ANYWAY
GG: so you say you have been talking to me from the future?
CG: YEAH
CG: MAKING PLANS AND WHATNOT
CG: TO PRY OURSELVES MUTUALLY OUT OF THIS MASSIVE MOBIUS DOUBLE CLUSTERFUCK.
GG: ok, so what is the plan?
GG: i mean, why did you want me to contact you at this moment so badly?
CG: OK WELL THE MOST IMMEDIATE POINT OF BUSINESS IS
CG: YOU SEE THAT GLOWING BLUE SCREEN BEHIND YOU?
GG: yes
CG: YOU NEED TO TURN THAT FUCKING PIECE OF SHIT OFF.
GG: ok, i can do that
GG: but why, what does it do?
GG: its been here my whole life and i could never figure it out
CG: I'M NOT GOING TO SAY MUCH ABOUT IT.
CG: BUT SUFFICE TO SAY THERE ARE JUST SOME THINGS YOU DON'T WANT TO SCREW WITH.
CG: THERE ARE OUTCOMES THAT ARE EVEN WORSE THAN THE COMPLETE ANNIHILATION OF EXISTENCE ITSELF
CG: FORCES MORE DAMAGING TO THE INTEGRITY OF REALITY THAN THOSE CAPABLE OF TURNING IMAGINATION INTO PURE VOID
CG: THEY ARE FORCES WHICH IF HANDLED RECKLESSLY WILL NULLIFY THE BASIC ABILITY OF INTELLIGENT BEINGS IN ALL REAL AND HYPOTHETICAL PLANES OF EXISTENCE TO GIVE A SHIT.
GG: i dont think im following...
CG: YOU DON'T HAVE TO FOLLOW
CG: ALL YOU NEED TO DO IS TURN THE THING OFF
CG: AND THEN DO THE NEXT THING I WAS TOLD TO TELL YOU TO DO.
GG: you were told?
GG: by who?
CG: BY YOU.
GG: oh...
GG: future me?
CG: YES.
CG: YOU COULD BE TELLING YOURSELF THIS RIGHT NOW, BUT WE'RE SORT OF WORKING ON A STRICT NO MEMO POLICY.
CG: WHICH IS YOUR IDEA OF COURSE.
CG: DID I MENTION HOW YOU DON'T LIKE IT WHEN WE ARGUE WITH OUR PAST/FUTURE SELVES? YES, PRETTY SURE I DID.
CG: SO I'M GOING ALONG WITH THE POLICY AS BEST I CAN.
CG: I AM BEING PLEASANT AND AGREEABLE, AND I WILL GENTLY LOWER A MAGNIFICENT, CORUSCATING COLUMN OF HOT FUCK YOU DOWN THE PROTEIN CHUTE OF ANYONE WHO SAYS OTHERWISE.
GG: uh... ok
GG: well it sounds like a pretty good policy to me!
CG: YOU DON'T SAY.
CG: SO ANYWAY, BECAUSE OF THAT, MY ROLE AT THE MOMENT IS TO ACT AS A SORT OF GO BETWEEN FOR YOU AND YOUR FUTURE SELF
CG: TO HELP ALONG THE PROCESS OF MAKING THESE PLANS
CG: WHILE YOUR FUTURE SELF IS DELIBERATELY VAGUE ABOUT SOME STUFF SO AS NOT TO "JINX" THE CONCEPTION OF THE IDEAS IN THE FIRST PLACE I GUESS?
CG: ALL WHILE YOUR CURRENT SELF IS NECESSARILY KIND OF DUMB ABOUT EVERYTHING.
GG: hey!!!
CG: SORRY, OK, JUST KIND OF IGNORANT
CG: BECAUSE STUFF HASN'T HAPPENED YET
CG: YOU KNOW WHAT I MEAN.
CG: IT'S NOT ALL THAT STRAIGHTFORWARD FOR ME EITHER, BUT I'M USED TO THIS SORT OF IDIOCY BY NOW.
CG: IT'S A LOT BETTER THAN THE MORONIC REVERSE CONVERSATION WITH EGBERT I TRAPPED MYSELF INTO.
CG: MEANWHILE TIME IS KIND OF RUNNING OUT HERE, WHERE I AM
CG: WE'RE COUNTING DOWN TO SOMETHING
CG: SOMETHING LOOMING ON THE TROLLIAN TIMELINE AND NO ONE KNOWS WHAT IT IS
CG: AND MY TEAM IS KIND OF FALLING APART
CG: I'M COMPLETELY LOSING TRACK OF EVERYONE AND WHAT THEY'RE DOING.
CG: SO AT THIS POINT I'M JUST GOING ALONG WITH WHATEVER THERE IS TO GO ALONG WITH.
CG: AND THAT IS YOU AND YOUR CRAZY FUTURE PLANS.
CG: AND THE SCRATCH.
GG: oh yeah! dave told me about that.
GG: what is it?
CG: I DON'T FUCKING KNOW!
CG: AT ONE POINT I THOUGHT I DID, I THOUGHT IT WAS JUST WHATEVER SENT JACK HERE.
CG: BUT CLEARLY IT'S NOT THAT SIMPLE.
CG: ARADIA KNEW BUT SHE DIDN'T SAY, AND THEN SHE WENT AND GODDAMN EXPLODED.
CG: YOU HAVEN'T TOLD ME EITHER, BECAUSE I'M NOT "SUPPOSED TO KNOW" YET.
CG: WHATEVER, I DON'T EVEN CARE, LET'S JUST DO IT.
GG: ok then...
GG: what was the thing i told you to tell me to do?
GG: right now, i mean
CG: OK, DON'T ASK ME WHY, BECAUSE I DON'T KNOW THAT EITHER.
CG: BUT THAT BLUE SCREEN THERE
CG: FIRST, LIKE I SAID, SHUT IT OFF
GG: ok
GG: then what
CG: THEN YOU NEED TO DRAW IT.
GG: draw it?
CG: YES
GG: and then?
CG: THEN NOTHING
CG: THAT'S IT.
#homestuck#karkat vantas#jade harley#homestuck act 5#page 3250#page 3251#page 3252#page 3253#homestuck act 5 act 2
2 notes
·
View notes
Note
Quick question, how many pages are there that feature kissing?
i excluded hs2 and also did not include a few panels from doc scratches segment where there were kiss panels that were both already scene and also very far in the background where it didnt really matter
apologies for any errors. i had to make this on desktop for image limits. problem? im a mobile baby
Aradiabot + Equius


pre and post retcon. page 2287
Tavros + Vriska

page 2380
Sollux + Feferi

page 2480
Jadesprite + Jade


pages 3252-3253
Karkat + Kanaya

page 3384
Terezi + Tavros

page 3384
Rufio + Hussie

pages 3391-3393
Snowman + Spades Slick



pages 3855-3857
June + Rose / Terezi + Tavros / Karkat + Kanaya / Jade + Dave
jade and dave dont touch lips here but she does still kiss him. page 3870
Gamzee + June
page 4944 ([S] DD: Ascend more casually.)
Dirk + Roxy

they do kiss but squarewave censors it. page 5238 ([S] Dirk: Synchronize.)
Jake + Dirk (Hal ig)

like do i legally consider this a kiss with hal or just dirk? funny how this is the only kiss in the unite and synchronize sequence that was not censored. pages 5249-5250
Dirk + Jane

again, they do kiss, but a fade to white censors the touching of lips. page 5252 ([S] Dirk: Unite.)
Jake + Dirk (Hal)

again. page 5252 ([S] Dirk: Unite.)
Kanaya + Rose


you were waiting for this. pages 5421-5422
Roxy + Dirk

page 5758
(Vriska) + Meenah

page 7351
Jade + Davepetasprite^2

page 8008. boob
apologies if i missed any. im 3 years old and have memory loss
#homestuck#OH FUCK I HAVE TO TAG THIS DEAR GOD#aradia megido#aradiabot#equius zahhak#tavros nitram#vriska serket#sollux captor#feferi peixes#jadesprite#jade harley#karkat vantas#kanaya maryam#terezi pyrope#rufio#???#andrew hussie#!?!?!??!?!?#snowman#spades slick#june egbert#john egbert#rose lalonde#dave strider#gamzee makara#dirk strider#roxy lalonde#jake english#lil hal#auto responder
104 notes
·
View notes
Text
baldur's hero
wc: 3253 au: baldurs gate au ch: xavier, benji
Xavier rarely goes to the courtyard without purpose.
It’s too noisy with too many people and never enough room to breathe—the restoration to the gate had been beautiful to witness. To be a part of, even. But years since the destruction and the noise has returned, like birds returning to the skies or brooks bubbling once more. It was in full swing everywhere but especially in The Heroes Yard. Blooming gardens surround marble statues, lovingly tended by a circle of druids that helped Baldur’s Gate and then never left the city. Their constant humming—occassional singing, even chanting—was the undercurrent to people.
He dodges a throng of young mages in electric colored robes, as they’re lead through a trail by a wizened teacher. She knocks her cane against a statue here and there, imparting wisdom to the sleepy group who follow dutifully. Xavier deftly bends and snags a scroll thats slipped free of one pupil. When he winks to her, she blushes all the way to pointed blue ears and covers her smile with a clawed hand. There’s not a hint of recognition about her silver eyes, just amusement and maybe embarrassment as she tucks herself back in with her group.
It’s nice not to be known. There is no statue of Xavier in this yard. But—he does find the one he’s looking for.
It’s only just past a lovely fountain. A popular spot, where people gather to idle free time. It is rarely empty. Sometimes, Xavier wishes he could have been part of the decision making process that went into this particular statue’s placement. It feels only right, after all, that maybe he should have been able to direct the artist who’d captured his husbands likeness.
“Sorry, I’m late,” Xavier says to the life sized rendition, taller than him only because it sits atop a pedestal. Benji’s pose is hilariously stiff, not just because he’s made of marble. Whoever had been commissioned to fill The Heroes Yard must have spent at least some time with Benji. They’d gotten the heavy set to his brow, the uncomfortable placement of crossed arms, his grimacing (but gorgeous) mouth. A stranger might look at him and find his stance confident, boastful. Strong in the face of adversary. Chin tilted back to survey the very city he’d saved.
Only, there has been an addition to the statue. A fuzzy black mustache made of felt has been taped to it, covering the natural stones rendition of Benji’s actual facial hair. It’s a bit lopsided, admittedly silly looking. Makes Xavier grin staring up at it. But it’s hard not to grin at Benji, even if this isn’t actually Benji.
He sits down at the edge of the pedestal, rustling through his coat pocket for the mutton sandwich he’d brought himself. It’s been hastily wrapped in yesterdays news paper, oil making it translucent here and there in little dots. They have too many copies, because Benji cannot stop himself from purchasing a page from every young busker on the street. So they mill about their home, hoping not just for a glimpse of the hero, but some of his coin.
“I always add too much oil to these,” Xavier complains quietly to himself and to Benji’s hero statue. “What I wouldn’t give for a curry.”
It’s been some time since Benji’s left, so he fends for himself in the kitchen. It’s a lonely part of their home now. But that’s Harper business. Xavier doesn’t ask. Not because he doesn’t want to know but—
They’ve had more than one fight about Harper business. The old argument that maybe Benji should retire, should simply stay home and find something worthwhile, something heroic here has been shelved for some time now. They don’t argue that one anymore, because Xavier understands that one better. The need to be doing something. The need to be helping. But the renewed and much debated (hotly, with both of them saying things sharper than they mean) is about Xavier’s safety.
Because is is safer for Xavier to not know the details. However, a part of him itches for someone to think of him as Benji’s weak spot and come looking for an easy belly to cut open. Xavier is no longer a paladin (if one ever stops truly being a paladin), but that doesn’t mean his hands don’t sometimes ache for the hilt of a sword.
The sandwich is still good, even if it has far too much oil on it. He leans back against one of Benji’s marbled legs, one of his own tucked up. He stares out across a pretty horizon overlooking the ocean that runs up against Baldur’s Gate. Xavier misses his tiny fishing village sometimes, especially when there’s all this noise (lovers laughing as they sit by the fountain and hold hands, a baby crying loud in it’s mothers arm as she shows the faces of countless, timeless heroes, the wizard and her students). He closes his eyes and enjoys the sun.
“Oi!”
Xavier blinks and looks to the side. Then adjusts his gaze much lower so he can look at this intruding stranger properly.
“You do that?” the tiefling looks furious, pointing at the statue he leans against. Xavier follows the child’s finger up to Benji’s face and the terrible mustache.
“What?”
“Y’think that’s funny then, do ya? Defacin’ a hero like that?” if Xavier were standing, the tiefling would come up to his waist. If that. He’s small, with just the barest hint of horns. A dark umber color, with dots all over his face and bare arms. His eyes are shockingly yellow, the kind that glow a bit when the sun hits them properly. Xavier tilts his head and then looks up to the statue, and then back down to the tiefling.
“This guy?” He jerks his thumb back at Benji with a smile. The tiefling’s face floods darkly, clawed hands balling into little fists at his sides.
“That guy! You new to the gate, half elf? That tief’s a hero, I said.” The child enunciates the word hero so hard it feels like he’s trying to cast a spell with it. He’s slight, but not not waifish, nor is he unkempt. Xavier remembers the refugees. No one could forget the refugees—no one with a heart, anyway. The outpouring of orphaned children, many of them just like this one. But Benji’s fan wears clean clothes and good shoes. His curly black hair is combed back, even if it also fans out around him messily.
“You don’t say,” Xavier ponders, glancing over his shoulder. He’s trying hard not to smile, brushing his hands together to clear his palms of crumbs. “He your idol or something?”
“That’s none of your business.” The little boy adopts Benji’s posture, arms crossed over his chest. He has a dangling earring that is silver, in an interesting snowflake design. Xavier slowly slides his way off the pedestal and stands. As he does, the tiefling child stutters back a bit. He blinks up and up until his head is nearly tilted all the way back—despite that, he still glowers, even if it’s less pointed now.
“What did he do that was so important?”
Xavier watches the tiefling climb his way onto the pedestal. He clings arms around Benji’s statue to keep himself upright. Xavier’s hands begin to raise on reflex, but he quickly lowers them when the child looks his way. However, when he turns back and starts awkwardly trying to snatch at the mustache, Xavier’s hands return to a safe distance. If the boy fell and broke his elbow all because of a mustache that Benji himself had slapped onto the statue, his husband would be distraught about it for weeks.
“They not teach history lessons where you’re from?” the boy asks, grunting with effort and an outstretched hand. The way Benji’s arms are crossed make it difficult for his short arms to reach. “Alright, how about this? A trade?”
“Oh?”
“I’ll tell you the story if you get this blasted mustache off him—s’not right! No one messes with the statue of Gale Dekarios.” He says the mans name with a haughty, sniffling air. Xavier has to bite his lip not to laugh.
“Not a fan of the famed Wizard of Waterdeep?”
“You wouldn’t get it. People are always tellin’ the stories of human men. All the time. Had to hear about them my whole life growin’ up. Even elves, yeah? Even half elves. No ‘fense to you.”
“None taken.”
Xavier understands what the boy means.
Gale was a handsome human man who did not want to save Baldur’s Gate—or maybe he did. Maybe his ideas would have saved the gate and the people within the city. But what would have become of the human man, with all that power? And when did Gale’s desire to save the city become more about wanting the power? No one else knew that story, because Benji was good. Benji was a hero, who didn’t go telling people the truth. That Gale Dekarios, whose statue was never defaced, wanted to take that stupid fucking crown for himself.
He breathes deeply to avoid letting himself get lost back in that day. It’s not what he’d come to the yard for. He’d come, because he’d missed his partner and wanted to see his face, even if it was a marbled version.
“Alright, son,” Xavier says, stepping forward. He takes the tiefling by the hips and gently picks him up. The boy weighs practically nothing and he’s easily set back down on the ground. He doesn’t protest. For a moment, Xavier can imagine a father doing exactly this. Taking a rowdy child and hoisting them around. There’s a twinge inside his chest. Children with parents. How special that it’s not a novel idea anymore.
“Tell me the story then. Benji, right? One of Baldur’s heroes?” He hefts himself up onto the pedestal and throws a lazy arm around the statue’s waist. He can briefly imagine himself doing the same to the real Benji. How warm he’d feel, snug against him. How good he would smell—like healing herbs and something spiced, like a hint of rain or the promise of rain. Xavier stares down into the statue’s eyes.
I miss you, he thinks fondly, smiling. It feels good to miss you, it reminds me of before. A letter sits inside his coat as well. Just like before. He’d meant to drop it at the post before coming to the yard, but he’d been hungry.
The tiefling boy begins telling Xavier the tale. Some parts are wildly exaggerated—Benji rode a dragon, he dual wielded maces blessed by Tyr himself (Lathander, forgive him, Xavier laughs internally). Some are painfully true, like his one mystical hazel eye, the long draw of a scar down the middle of it.
“Mm, he didn’t get the scar from the eye,” Xavier comments softly, finally plucking the mustache free. He cannot stop himself from pressing a swift, chaste kiss to the statues cheek and then hopping down to the ground. The heavy sound of his body makes the tiefling jump back, though Xavier lands perfectly with knees bent. He rises slowly, holding up the mustache with a toothy grin. The boy is blushing even harder than he was in anger.
“He’s married, y’know,” Benji’s fan snorts, pointing to the statue. “Heard his husband’s ferocious—seven a half feet tall with a sword that calls lightning. They say he killed Ketheric Thorm—but I don’t believe that.”
Not just me. It is rarely just one person who kills a God.
“That’s good. Shouldn’t believe everything you hear. It was Dame Aylin that killed Ketheric.” Let her have the glory; she deserved it. Xavier toys with the plain silver wedding band on his finger. He feels a roll of nausea from the memory of Ketheric Thorm, but it is an ancient hurt, a cold and dead fear that he’s mostly grown free of.
“No. It was Karlach Cliffgate—you’ve pro’lly never heard of her, ‘cause she’s another tiefling.” The boy turns his nose up, snorting contemptuously. Xavier does not tell the young boy that Karlach had not been there for that particular fight, but instead a powerful and terrifying Githyanki woman, who stories do not tell of frequently enough for his liking. But that was history.
Favoring the Gale’s of the story—even glorifying Xavier to a seven foot lightning wielding paladin, though nameless as he was.
“You know,” Xavier says contemplatively. “I bet, whoever keeps putting these up there does it early in the morning. Probably right before dawn, so no one can see.”
His thoughts ease into the memory of Benji, the sunlight not even peeking over the horizon yet. The window to their bedroom open, because they’d secured a spot by the water and the smell of it comforted Xavier. Their hands on each other, touching faces or sides or arms. Small kisses while Xavier is half dozing still, almost asleep—Benji’s leaving, is telling him he’ll be back soon. Telling him to write, telling him he loves him.
The boy looks struck by the idea, his grin going sneaky. Then he schools it neutral and huffs.
“Not thankin’ you. Was an even trade. Information for help. That’s fair by Baldur’s ways.” Xavier bows deeply, making the boy look instantly sheepish. He turns to run, down a winding and flowered path. At the end of it sit two tieflings, a fat and happy baby in their lap. Xavier watches the boy crawl up onto a stone bench, whispering conspiratorially into a mans ears. The tiefling is the same shade, with the same spots.
Xavier lets himself have one last look at Benji’s statue before he leaves the garden.
—
Finally in his hands once more, Xavier does not let Benji go again.
Not for the entire night. There is no moment where he is not touching him; from the exact second Benji crosses the threshold to their modest home, Xavier’s palms slide across his forearms, to his shoulders. Their mouths crash together in a desperate, laughing kiss. Benji is lifted off his feet, crushed to Xavier’s chest. His armor clinks. The smell of leather oil and dirt, but also Benji.
His hands stay when they take a well earned bath together in a washing tub that they’d specifically bought for this depth, this width. To fit the two of them. Hands touching while they’re in bed, and not necessarily just for the sex that they have. That ranges from rough and needy and desperate and wild to slow and languid and sore and tired. But his hands stay even after that, just simply cupping ribs. Running over a broad torso, a hairy chest. His fingers roam until they find—
“This scar was not here before you left,” Xavier snips, pushing Benji to his side to stare down at the small healed wound on his side. It’s a tan scar on dark skin, no longer than his finger. It’s minuscule in comparison to the one on his back, or another on his hip, or the burn on his calf. Xavier peers down at it with narrowed eyes. The black kohl he paints around his eyes has run horribly and Benji’s cupped hand on his cheek brushes a thumb through it.
“That’s always been there,” he argues innocently, with wide eyes. One black and beautiful and the other hazel and ethereal.
“Fuck you,” Xavier seethes with a laugh. “I know every single scar on you. I’ve tasted them with my tongue.” He punctuates that sentence with a flat lick to this new, offending scar. It makes Benji shiver, his hand clutching harder around Xavier’s cheek. His other finds a home in his hair, carding through the long red strands.
“Arrow grazed me, s’all.”
“Archer dead?”
“If I said he weren’t?”
“Suppose I’d take my Oath up again and find him and shove an arrow through his fucking—”
“Archer’s dead,” Benji laughs, pulling Xavier closer for another kiss. It doesn’t stay gentle, though it starts with just the press of lips and a sigh of air. It deepens with both their mouths opening wider, their tongues rolling and sliding against one another. Xavier moans into the kiss, sliding himself until he’s entirely over Benji—and his hand stays around this new scar he has to memorize. They kiss until it’s messy and when they part, a string of spit momentarily connects their mouths. Xavier licks it hungrily, greedily, eyes hooded and it snaps.
“Death of me,” Benji mutters dramatically.
“Swear that,” Xavier laughs, ducking underneath Benji’s chin to kiss his fuzzy jawline. He moves until he finds his pulse. He sucks it hungrily, thinks to leave a long lasting bruise so that anyone who sees the Hero of Baldurs will know that hero does have a terrifying, greedy husband.
“What am I swearin’ to?”
“Your death is to me only.” Xavier pulls back. Their breathing has both gone harder. There is a flicker of Benji’s youth around his eyes; but they are both so undeniably older now. Gray to their hair, wrinkles at the corners of their eyes, scars everywhere. “An archer can give you a scar. Maybe some Zhentarim fuck surprises you with a dagger—maybe you come home with a scar here instead.” Xavier cups underneath Benji’s knee, touching the soft skin that is never touched by anyone but him.
“But you swear that, Benji. No Harper business takes you from me, I’m there the day you die, or you don’t fucking die, got it?”
Because it all felt unfair sometimes, for Xavier. The city got it’s statue. Boys got their heroes. Harpers got their cleric. He leans forward until their noses are nearly touching. Benji’s eyes have gone dark. Possessive. His hands touch Xavier’s lower back and shove firmly until they are touching every place they can touch.
“Swear,” Benji says in a husky voice.
—
“Tyr’s fucking greatsword,” Xavier moans through a mouthful of food. Breakfast sits, hot and loving prepared on their kitchen table. It’s wooden and long enough to fit company, when they eventually have company. That morning, it is only the two of them, Benji sitting on one side with a mug of steaming tea and a satisfied and sleepy expression.
“I missed your cooking.”
“Could learn to do it yourself.”
“I made sandwiches.”
Benji’s head rolls back with a loud crack of a laugh. Xavier has never heard him laugh like that around anyone, save maybe Maran. Lark’s never gotten that laugh—Benny’s never gotten it either. Matilda gets his soft, snorting laugh when she’s making too mean of a joke. Nettie gets his chest deep chuckles, whenever they visit the grove. Children, that swarm him in droves on the street when they recognize who is he, get humored, if not sometimes awkward laughs.
Xavier scoops more food into his mouth, goes for quick sips of the slowly cooling tea. If he were in the right frame of mind (certainly not the messy, debauched, fucked senseless and tired version of himself that finds getting out of bed harder and harder with every year that passes) he might have ruminated more on that laugh. On how much of Benji stays his, despite how much of Benji is also for others.
Instead, he clears his plate and flips the sign on his blacksmith shop to close—and they spend the evening together, the windows shut to the noise of the city.
6 notes
·
View notes
Note
Okay try this one on for size loamhead
Hex:
tp0b0bwpngrm0bac0jlosulpxe8vfay0tejnjnz12fnr48d1tloqi26u998br4ap62op9q7x38zbrvg8kn5yfsd0xbp3a9czfbkydpowvb6hdbuvhxzo0c3wp4xgy8r4wy0we8hfwhoym9tqdmqjkwj3mytiubsojvbjnwt5yq2z7yu6mgmgemac8yki18afvzncgtnaqqyng0egkk59wovp6pr96emzeq4iv5lalzfgpwnrzlitdyjgk7olr83vdjtdd7s0j9pkoqg0wk4l8tcxcfysrxc4mq46ildhm30akheazz8j8l32puzsp3qe0zqrgq5w4v6x0l70wzof1k904qsu91fycqgen1g0ej9tz7169bw8uer698js08qndtsy35vx31xytfco8iu9m05ovo8ohdh76x5agrgghtmq32q98jfu9fn09nm9z9o5i8j6lhmgzi4t681hosplrvt6ioxu7zkmm8r0yd1seitsy6imlmjl5vylh9v7q7bucku72yjaknom61251osee03qgho0eruynss69t4ub1oabtvavitca5ftyl3715i6iyumgo6qfie70umkv77qmk4b79z2y71q31pxrummb5j7v64zpsbj64lhx4u939ebl6qpvnp8d87k3ngcmoe146ilurres6fhyuang64s6jgu8zentepcvunjpuwupul875mwak9p4jb7cvfcc4u11qmyl7d90ilys95bj44kw2e8anw9v072ufxqvhlg53kpfsx5i1jq7xkydgh4vo5ac763vear2p3d7zyzhzpvv0x66vlezahsw3cv3tr502yy78rmuw22yt2b9ck2oiy1pdj7zkfbfhknk7vc2k8jufv2blm9xx9wa7y2ux6e8iz063v0yq3ffjp6tvq9mjs89h4v5u4dr6320j107c75ris4egi6ieik9gi3jqk49rsh84grll12cndnfiwoxw7yxac54pxfap1zruvj4n0stfdacckhlh747x7gny2kb0yka31dz6e946t8k8t5skw8x0qfuxfabmyc7nhk411a1b7vu3vsfq4sxh0ih6of8p4d1ndrvqhcrsde65t66xotsbbliid1u86kjz6axvcgdnl37883otzwwm9orhw4t3cse0ymg3h1ycfe1ls73aukoytlyxt4uwxgwaj16cjepl39v7v048a1hnoxtf6d1vv5a67sygdaseaokcb831g8cxucajsuy4lhv3bez5va69l07gdapzv983204tp5x1rb6rv4lny26aca2vxo40gd0sah86kw0wf0yy2jdh3lb9ki33dccqg4fimvbfz53gyads9kmytn76v1r6tx1668zcb6mj9s6ytfgzl92xefhyr1efql3td3ja06a8a1s08rmvppq1hmw4h8f5x40w15tgrfcxskehbup4mrpl5mfghtmeuy6r7ceu66o25rr98vqxctg0m33svoikgsujv8z0s96jywv4f05dsrq851fsid12e3cr4ff0efhgxc6q0egfxqhfuhehfvqdsok74mz98utvmyvte4pz409up9coqhvhnt3jmdyflqilw52pzzt4q3gfb701mju8tlqslhovnrp08ex48mf9vmp09ojmbdvc83qaex6tqai7vam4rvyc4irxv9yefkfo3pw65lp5u867hhygjik549qj77ayhls0sz4hg5ncygjpgso3vpgblmvfyxgz7iyby2de40bwzyjjk2ruayodbhfkw83ozs7a7lblmk35u9bkr5fp59h11vzfa0a2sykhgalh5onw2o1g8zhje92ub2cb7jn2mwg3ol6o4ko4m1whj415rw3ddzk3dubq569avifxj5060zu20ca3kd6ngvcpfe8ke06exrra86h7ocw74xqhn5o9hoyzchhw8zhaezexnwxsvcpu18b6ptr8sn8ilnap8v34tjug97cced9oc7pc3bl811t4ybxx5bgorss270zu8z7vu90e6myn77xaji7vzou4p1x0988mgar26mhn2i5t2sszefmystr0ebp2pybv0x3bqqngqda8tasaiqeuyryrzg0i6s35jmkmw8l0w6n97ok2st8vimo1ga7wcqnxnv519o0l2ofzhw6848rbq4fnkb2irtrwuecn4q62cy2sjbfg3vzs8b090b3efgqup2d4yzgf2zyt6zshbtlubhtwlufoag5udfce92yr1dvna0dxw1057rezvsscuz1hlagx48kqyqiqm88zqafd2lg283kgoey5i7prrsh5qxqx0mluh5civhnsv6slor6cnfud0ljvz0bdgeqly567otnjed4q7y7yr9j0mp0t3uew4p03bu8984q8htkp17jchmfx8cv15vfej0tar7dy3nmqrqvx4botje817yduswm0vxq6axr07tcuf39uy69d7d48inyu1sxhic4115ufr7i2vpafk5nt270s0v84cn1vb5105mzi5kosnok7l1m4otbyboq93nx074jny10w5zv5z0w1ythc48d68trpebaj6icgfer8rd8yt89eocgkkelibvk6aagmisoqxdd9uxqqq4g1g1tuf20h0mqn0go6209hmfvry99wedzpp0sj8g21e91la9z3fwsofa08zt2zkwcflbv3nmsfuk5hd3cpurfrurnuzlrmhpessu4s28p0peyohl9uc48j5q3107fz604q9lj85b6cslkesjldqo8yu14c1mpom3gyxiu3rfhjadu8420idjsgqnp8tmzw5b46ubj6kdpi9nn2x8nwvx38b9ntnaw7jnfge9ai57bkfjjpa320enrxevsh7zgn4idwm360hasa3ntagtvg84hq1yddgil42i0ew1k0lq20nkpz4akbqcrx6ws9t7wjv5dnuibsdvcnutwkp1llqr1fm8ubk2gwi7w2rj8068xpc9jortrglum65zqk11i3w9qcjf3jsd6g4iv9fw7y18vo862kb241ztz8nzw5d3x7kme5bfnexhg0chax0i6ij9kt633yuaww5p671jw0ggkmfmbrzc001svzqd8u05g1f4ahnz72op44n00fwnindxo17n7oe71ec637ld9ku0sg8wdfbskogk1ghoj9s4irnjx01vhk5tx0q5j2hovfckkynh0jj1rm3ehrihdt8ocp6v5eb1ayof8y5dkkruximjyed70e8q9fuhzsjx7w6l82jw0
Wall 4
Shelf 2
Volume 6
Page 216
library of babel website allows hexes up to 3200 characters long, this one is 3253
2 notes
·
View notes
Text
Trans-friendly Mods for DAI (Guaranteed to piss off terfy templars!)
As a mod enthusiast, I’ve combed through most of the Dragon Age mods that are out there. When working on an explicitly transfeminine Lavellan (yes, you can simply headcanon your character as trans, but it’s not quite the same, is it?), I gathered all the mods that allow for better customization of gendered traits, along with a few decor mods to reassure everyone that your unchecked paramilitary spy network/cult supports trans people.
Enhanced Character Creation - Removes most unnecessary restrictions on character creation, and adds a little more customization for things like tattoos and hair colour (which can now be dyed a wide range of at least two flashy colours at once - this absolutely allows Trans Pride colours!).
Note: This includes unlocking all voices, but it conflicts with the main files for Any Voice. (It doesn’t conflict with the combat exertion noise fixes, which are in fact necessary if you choose a voice that’s normally locked).
https://www.nexusmods.com/dragonageinquisition/mods/2707
Any Voice - A set of mods that allow you to use any of the four VAs regardless of gender (and change the combat noises your Inquisitor makes, which will be a different VA if you change the voice but don’t use these!) Any gender-specific lines will simply be unvoiced. The main files conflict with Enhanced Character Creation; the exertion changes do not.
Flipped Pronouns (on the same page as Any Voice, but very distinct effects and worth listing separately) - This file, towards the bottom of the Any Voice page, flips the gender flag of your Inquisitor, allowing you to select, for instance, an “Elf Male” body type while being registered in all dialogue as female. (No other genders/neutral addresses are scripted, so you are still limited to a binary choice). This does affect romance options but does not affect Codex/War Table text.
https://www.nexusmods.com/dragonageinquisition/mods/3108?tab=description
LGBT Heraldry - Replaces Templar heraldry with your choice of pride flags around Skyhold, including in Cullen’s office. Let Popular Video Game Character Cullen Rutherford celebrate his VA’s trans friends that he’s always bringing up!
https://www.nexusmods.com/dragonageinquisition/mods/3253
Clown Cullen - Exactly what it says on the tin.
https://www.nexusmods.com/dragonageinquisition/mods/2929
The Peacock Throne - Replaces Circle throne with a glorious peacock throne (peacocks being the iconic trans bird).
https://www.nexusmods.com/dragonageinquisition/mods/1547?tab=description
229 notes
·
View notes
Photo
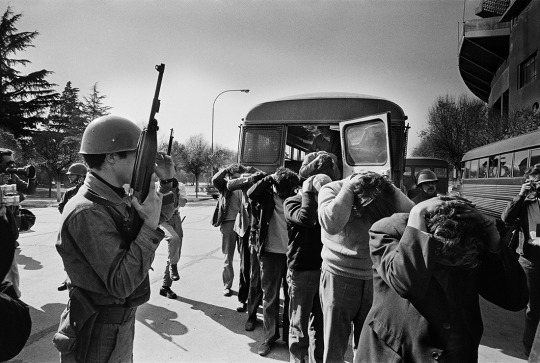
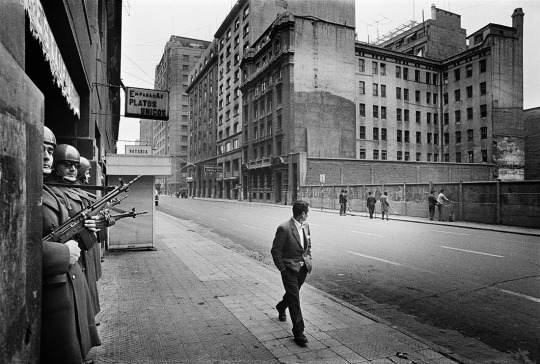

Chili septembre 1973 Koen Wessing
http://www.jeudepaume.org/index.php?page=article&idArt=3253
2 notes
·
View notes
Photo

本日は、眠眠打破キャラクター「打破山眠太郎」について。
眠打破ゼミナールの予備校講師。 教育熱心で親御さんの信頼も厚い人気講師。 特技はペン回し。
https://w.atwiki.jp/yurupedia/pages/3253.html
22 notes
·
View notes
Text
Mine ~ Gilbert Blythe AU

Request: Request for Gilbert? The reader is best friends with him and they’re in college. Gilbert gets jealous because she’s spending time with another guy helping her in a class, and angst and fluff and just the classic trope of their feelings being revealed eventually? 😊💓
Summary: Gilbert had known Y/N his whole life, and for just about that long he’s been in love with her. Now they’re in college together, and Gilbert’s feelings have only grown.
Fandom: Anne with an “E” (Anne of Green Gables)
Warnings: jealousy, unwanted glances, mentions of sexism, super cliche at the end lol sorry not sorry
Word Count: 3253 (9 pages) issa long
Date: November 11, 2018
A/N: hope this is ok, I worked really hard on it. Feel free to leave your feedback or other requests. Taglists and requests are still open, never be afraid to ask! Hope you all enjoy and happy reading!
Also, John is Y/N’s study partner.
~Ciara xo
Y/N L/N. The only word he could think of to describe her was perfect.
For as long as he could remember she was in his life, holding his hand lightly in her much smaller one, her head resting on his shoulder. The image of them in that position in so many of his memories as he flashes through them, giving him a feeling that he's become so familiar with. It sent goosebumps down his arm, makes his stomach do flips, his mouth to go dry. He's felt this way for so many years, but never realized what it was until that day a few years ago, the day his dad died. Once again, an image of their stance appeared as the flashback played in his head. He could almost feel the light misty breeze of the Prince Edward Island beach near their small town, Avonlea.
"Gil?" her voice was so soft he hadn't even heard her, his own thoughts clouding his senses, his eyes caught on something in the distance, but he didn't know what. The light squeeze of her hand in his brought him back to her. As he looked at her, resting her head on his shoulder, he saw her E/C eyes already watching his own hazel ones. Her other hand came up and lightly caressed his face, fingers so cold from the dead winter.
"I'm sorry," he said, trying to hold back tears, leaning lightly into her hand. She sighed sadly and shook her head, taking her head off his shoulder and her hand of his face, grabbing his other hand as she stood in front of him. She gave him a light smile, and he could tell she was holding in her own tears.
"No, no. Don't be sorry, Gilly. It's ok," she whispered. "I was just saying that if we stay out for any longer we might get frostbite. Besides, dinner should be ready soon, and we ought not to be late." She looked into his eyes, but it seemed as if he looked right through her. He looked back out to the ocean, seeing the sun hit the horizon.
"Can we stay, just a little bit longer? Watch the sunset?" He asked, looking back at her. He looked so desperate, she couldn't say no to him. She smiled and nodded, wiping a stray tear that fell down his cheek. He pulled her closer, into a tight hug as she lay her head on his chest and they watched the sky turn many pastel colours until it went almost black. They didn't know how long they stayed like that, watching the sky, listening to the crashing waves. Once the sun had disappeared from sight, the pair started to walk home in the darkness. They reached the part in our path where they parted. Gilbert begrudgingly took his hand from hers, saying goodbye and beginning to walk away.
"Gilbert Blythe! Where do you think you're going?" She called after him, an honest confusion in her voice. Gilbert seemed just as confused as her.
"Um.. home?" he replied. Looking back at the path behind him that lead to his farm. To be honest, he didn't want to go back there, he didn't know if he could. After all, that's where Y/N found him. After the funeral, he hadn't come back to the house, which worried her, so she went looking after him.
"You know I will not let you stay by yourself, especially after.. everything that.. happened today. We'd be more than happy than to have you over for tonight Gilbert. For the next few nights even." She said walking over to him and grabbing his hand in hers again, dragging her down the opposite path that leads to her house. "Besides, I need my knight in shining armour to protect me from the horrifying darkness of night." She giggled and looked back at him, eyebrows raised. He smiled a genuine smile, the first one in weeks, giving into her and letting her drag him along. She took his hand and swiftly put it around her shoulder, so his arm wrapped around her.
The knight in shining armour was a reference to when they were children. She would play the beautiful damsel in distress, waiting for her handsome prince to come and save her. And, to no one's surprise, that was Gilbert. Sometimes, she would get bored of always being the one in trouble and make Gilbert the princess stuck in a tower, wearing one of her dresses as she stole one of his sweaters and galloped along on the broomstick-horse, coming to the rescue. The memories, still so fresh in his mind even if so long ago, made him chuckle.
"Oh my goodness, Y/N L/N! Where have you been, young lady?! I've been worried sick! You missed dinner, so it must all be cold. You've missed all of your chores, so you'll be doing extra tomorrow, the second the sun rises!" Y/N's mother ranted as she put her dish towel that was hung over her shoulder on the sink. She came over and slowed once she saw the young boy beside her, still holding her daughter's hand. "Oh, Gilbert. Hello sweetie, how are you doing? I wasn't expected company, sorry the house is an absolute mess. Come in, come in, before your ears fall off! I'll put on the kettle." She smiled and rushed back to the kitchen.
Y/N and Gilbert, shaking intensely as they sat by the fireplace for warmth, sipping the scorching hot and slightly burnt tea made by Mrs. L/N, a giant fluffy blanket coated the two. Mr. L/N, Y/N's father, gave him a pair of his pyjamas to sleep in for the night as Y/N's parents sent them up to bed, giving Gilbert the guest bedroom across the hall from Y/N's bedroom. As they crept up the stairs, careful not to wake up any of her other many siblings, she took his hand and dragged him into her bedroom.
"Y/N!" Gilbert whisper-shouted at her. "What are you doing? I'm not supposed to be in here! A man should never be in a young lady's bedroom, especially at night. What will you're parents think? I'm not-"
"Gilbert be quiet! Before they hear us!" Y/N giggled, covering his mouth to stop his ranting. "There's nothing wrong with you being in my room, you've been in here before."
"Yeah, when we were younger, much younger. Now it would be frowned upon." He started up again. She rolled her eyes, setting a few blankets on the floor and one of the pillows from her bed, pointing Gilbert to it as she climbed into her own, obviously old and almost at breaking point bed.
"You're sleeping here. I'm not leaving you alone." She said, her voice going deep, serious. Something that wasn't usual for the smiley girl. "Gilbert Blythe, I sure hope you know that I swear upon my life that I will never leave you. And we will always be together, forever. I swear it until my dying day."
The feeling, that one mentioned from before, had become so intense at that moment he surely thought he must've become sick. She leaned down from her bed and placed a light kiss on his cheek, before placing her nicest duvet (which wasn't that nice, but he wouldn't complain) over his still shivering body, but this time he was shivering over something else other than the cold.
When Gilbert was young and asked his father what it was his mom was like, he would tell the boy about how she made him feel, whenever he saw her, held her, the undeniable feeling of love. He never quite understood the concept of butterflies, for how could such creatures even make their way into your stomach and still flutter around? But at that moment, in her bedroom as the warmth of her lips still lingered on his pale pink cheek, he understood everything.
He was so deeply in love with her, it almost pained him. But it did especially at this moment, almost 4 years after that night, and he still hasn't said anything. Which he thought to lead him to this moment, he should have expected it.
He was now at the age of 19 years, studying at the lovely Queen's Academy to chase his dream of becoming a doctor. Y/N was just about 17 and had been, much to her and his delight, also been accepted into the academy to study to be a nurse. That, of course, wasn't the part that had hurt, but the sight right before his eyes, an unknown man with his arm around her shoulders, like he had when they walked down that path, looking at each other, giggling at something, he couldn't tell what.
He felt honestly betrayed. She had never been exactly his, but he still felt as if she had left him, forgot about him and their promise. But mostly he felt angry. Not at her, he could never be angry at her even he tried (he knew from many personal experiences), but from that stranger that had taken his girl away from him. He took his book and checked it out, trying to avoid their eyes, but of course, to his luck, that was no use. He heard her call out his name before he slammed the door shut of the recently quiet building.
"Can we pause our session just for one second? He's my best friend." She smiled sweetly, taking his arm off her shoulders and looking back at the door he had just left out of. He nodded, sharing his own smile. "Ok if I'm not back in ten minutes you can leave! Thank you again so much for the help!" She called behind her shoulder as she ran out the door, tripping slightly every once in a while on her heels. She saw Gilbert's unmistakable mop of curly black hair walking just ahead of her, so she jogged to catch up with him. She tapped his shoulder, smiling a great smile as she linked her arm with his.
"Hey, Gilly! I didn't think you heard me in the library just then." She said, trying to get his attention, which was still focused on the path in front of him. "Gilbert, what's wrong? You've been acting so... distant lately," she sighed, pulling him to the side, to get out of the stream of walking people. He turned and looked at her, instantly feeling bad by the look of desperation on her face. He smiled at her and placed a strand of hair behind her ear gently, making her blush a little bit. Thankfully the red of her cheeks could be blamed on the cold winter.
"There's nothing wrong, Y/N. I'm fine," he said softly, trying to continue walking, but she wasn't having it. She grabbed his arm and brought him to a nearby bench, forcing him to sit.
"Gilbert Blythe! I know that isn't true, you know I can see right through you," she said grabbing his hands. "Please tell me what's wrong, I'll do whatever I can to help, I swear it." That look alone that she gave him almost made him cave right then. Almost. He knew he couldn't risk all those years of friendship over some silly crush. A crush that just won't leave him alone. He took his hands away from hers and got up.
"Sorry Y/N, but this isn't a problem you can solve," Gilbert said, turning his back to her, knowing the look of hurt that would be on her face about now. "I just need some time alone, away from you. Goodbye." It took everything in him to walk away from her and not turn back.
The next few days, Gilbert did everything he could to ignore the girl he cared so much for. He knew that she'd do anything she could to find out what was burdening him, and he knew he couldn't say it was her. It had been a few weeks since he last saw her, and it was an understatement to say he missed her.
He had seen her more and more at the library with that man. He couldn't help but feel as if he was being replaced every time he heard her beautiful laugh pass her lips, because of him. He tried to avoid the general area, but it was like he was drawn back each time.
Little did he know that Y/N was in just as much pain as he was.
The past couple of weeks without him had been much too bland. She would only leave her small shared apartment when she went to her study sessions with John, in the library. And even though he was nice enough and made her laugh, he wasn't Gilbert Blythe.
She had tried aimlessly walking around the Queens Academy campus, in hopes of finding him, maybe sitting on a bench, reading a book. But she had no such luck. After all, it was a very big school, with many people. Many more than in Avonlea.
But she was truly hurt that he had, as it seemed, completely blocked her out. She still had no idea what she had done to cause anything upon him. And the idea of causing such a pain unto someone she loved so much had burdened her very much.
She was out on one of her walks again, it was getting cold outside, small snowflakes fell quietly from the sky, landing in her hair and on her face. She felt as if she was going to catch her death at any moment.
John had caught a cold and wasn't able to make their study session, so Y/N was off to the library by herself. She was a bit nervous, walking by herself in a campus ruled by men, some of which with bad intentions on a pretty girl like her. Her eyes constantly scanning her surroundings.
Thankfully she had safely made it to the library, with no trouble, but some unwanted lingering stares, but she had expected it.
"Why, good afternoon Y/N, " the old librarian, Mrs. Dell said kindly. Y/N smiled and nodded politely, giving her a nice hello as well, before heading off to the books.
Gilbert froze up immediately when he heard the name pass the old lady's lips. He heard her dainty footsteps walking slowly towards him. He wanted to run but it was as if his feet were planted to the ground, since he knew that he did want an excuse of seeing her again, even for a second. His back was to her, and he had hoped that that would be enough for her to dismiss him.
Of course, he didn't have such luck.
"Gilbert?" Y/N's voice was quiet and unsure, but the raven black curls were hard to miss, especially to someone who has become so familiar with it. Gilbert didn't change his stance, so Y/N walked forward and grabbed his shoulder, making sure that this time he wouldn't escape. "Gilly, please, can we talk?"
He didn't look back at her, it took everything in him to keep his gaze ahead. He could hear her sigh and feel her hand travel from his shoulder down his arm to his hand as she pulled him out of the library. He was shocked but didn't bother fighting it. She nodded at the librarian as she headed out, Gilbert being dragged not too far behind, earning a strange look from the kind old lady.
Y/N pulled him closer to her side, constantly checking her path and using him as a human shield from the lingering stares. Gilbert realized the odd behaviour, and also looked around, wondering why she was being so cautious. Probably because she doesn't want her new boyfriend to see us together, he thought to himself but didn't dare speak it aloud.
"You know, even if you refuse to talk to me, I just wanna say that I am thankful I found you. I was starting to think you left. My, that would've been torturous. You're my only friend here," she says quietly, squeezing his hand. He looks down at her, seeing that she was already looking at him. Their footsteps slowed to a stop as they looked at each other, both trying to hold in tears.
"Surely that's not true. I've seen you around with other... people," Gilbert states blandly, breaking eye contact and looking over her head instead. She laughed.
"Well, maybe the only other person would be John but-"
"Yes, John," Gilbert interrupted her, looking back at her. "I thought you two seemed quite close. That's splendid." The last part of his sentence wreaked of sarcasm, telling her that something was up, and she thought she knew what.
"John is my study partner, Gilbert. We were paired up together since my professor thinks I can't handle my own work due to my.. well, gender." She rolled her eyes and crossed her arms, thinking of her nuisance of a teacher, who was too much like her old one in Avonlea, Mr. Phillips. "Besides, why are you getting so worked up? I've seen you with many other people and I've said nothing." Gilbert exhaled and pushed a hand through his messy curls.
"Because it's different, okay? I don't like seeing other guys like that around you. I don't want them to take you from me." He stated, not being able to look at her, his cheeks starting to burn up from the confession.
"Take me from you?" Y/N asked, slightly offended. "Might I remind you, Gilbert, I am not an object that you own. I am-" Y/N started to rant but was once again cut short.
"No, Y/N. Not like that." Gilbert said, taking her cheek in his hand. "I don't want them taking you away from me when I haven't even gotten the chance to make you mine." He couldn't believe what he had just said, and as it seemed, neither could Y/N. Her mouth went open, trying to think of a response, but nothing that could truly express her emotions came to mind. So of course, she didn't have to say anything and just kissed him.
She kissed him hard, everything breaking loose from their chains. And sure enough, he kissed back. They didn't care that they were in the middle of the campus, probably many nearby people watching in on the affair. Nothing could break the moment they had waited so long, too long, for. The butterflies from Gilbert's father's stories seemed to have tripled on their effect, as well as so many other things, as their lips moved in sync, slightly chapped from the cold. They broke apart for air, not moving too far apart from each other, placing his forehead on hers as she giggled, sounding like a wind chime.
"You were always mine, Gilbert Blythe. And I will always be yours," she whispered to him, looking him straight in the eye as her contagious smile grew a little bit wider. He smiled back, so big until it started to hurt his cheeks, and grabbed both her hands, pulling her in again and placing another kiss on her lips, guiding her hands around his neck, then placing his gently on her waist. "Until my dying day, I swear we will always be together."
And suddenly, John didn't seem that important anymore.
#gilbert blythe x reader#college au#au#anne with an e#imagine#oof#gilbert blythe#SEND REQUESTS#anne of green gables
345 notes
·
View notes
Text
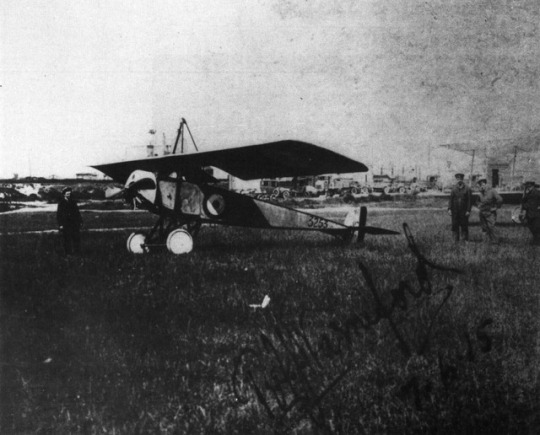
Opposite page: Above, members of No. 1 Squadron RNAS pose proudly with 3253 at St Pol aerodrome. (Albatros/PL Gray Archive)
Photo and caption featured in Windsock Datafile No. 016 - Morane Saulnier Type L by J. M. Bruce
6 notes
·
View notes
Text
Space Between (7)
*****Tag notifications aren’t working so for those who don’t know, I update this story on Wednesdays. Your best bet is to just check for the newest chapters on Wednesday evenings. :/ At least, until Tumblr gets their shit together. Smh.*****
❤️ #BunBunWednesday ❤️
Words: 3253
MASTERLIST
TAGLIST: @katshrev @elaindeereads @soulmates8 @naturallyqueenie @onyour-right @msincognito67 @janellemonaenae @afraiddreamingandloving @hutchj @90sinspiredgirl @airis-paris14 @dolphinpink310@purplemuse @purplemuse @amberkay284 @leafdragon117 @meeky-imagines @aieyr @h-challa @quietemptydiariess @katasstrophey @wakanda-inspired @destinio1 @dessianna1 @blackpantherimagines @httpjex
Space Between (7)
Y/N was avoiding T’Challa.
She’d been doing so ever since she woke up and carefully lifted Bunme out of his bed to prepare her for another day at school. She’d had breakfast delivered to their room and stayed in their even after her daughter’s departure. She wasn’t sure how long she could avoid him but was pleasantly pleased with her success thus far.
However, she realized that she needed to seek out Nakia and ask the woman about possibly accompanying her to Jabariland to go visit Hawla later that day and could not figure out how to work her Kimoyo beads.
She was walking down the hall, about to send up a prayer of gratitude for the continued avoidance of a certain king when she felt herself being grabbed.
Damn
“We need to talk.” She tried to not focus on how good he looked, smelled, or how his touch reminded her of their events just the night before. So passionate, so fulfilling.
As much as she hated him at times, she could never deny that the man always satisfied her every desire under those sheets.
“About?”
“Y/N.”
She jerked her hand back out of his hold, prompting the king to sigh. “Personal space, T’Challa. Personal space.”
“You really want to talk about personal space?” He propped a brow which earned a small glare from the woman.
“What do you want?” She relented.
“Why have you been avoiding me?” His handsome face took on a small frown which elicited a look of shame from the princess.
“I haven’t-“
“Y/N.” His voice indicated that he was in no mood for her sideways excuses.
“It was a mistake.” She said rather loudly. “We shouldn’t, I shouldn’t have, I don’t know.” She stammered, placing her middle and index finger on her temple. “I never should have come to your room, and I want us to just, to just forget it, okay? Let’s just pretend that it never happened. Alright?” Y/N went to walk away, but T’Challa grabbed her, pushing her up against the wall. “What the hell-“
“How much longer do you think you can hide from me?” He questioned darkly, his voice a mixture of frustration and desire.
“Let go of me-“
“Answer me!”
“Need I remind you the last time you neglected to heed my warning!” She hissed quietly, struggling against his grip on her wrist.
“Run? Just as you always do.” He shot back smoothly, remaining stagnant in his spot.
She tried to lunge at him, but his grip was iron. “I’m right here, T’Challa.” She sighed, letting her eyes fall on their connected hands. “How the hell am I hiding?”
“You know what I am talking about.” His voice dropped as he lowered his mouth toward hers.
“What are you doing?” She whispered with pure unadulterated apprehension, inhaling sharply as he quickly diverted his lips to the middle of her chest.
“Why do you continue to deny yourself?” He questioned against the top of her breast, sucking the supple skin that was pushed up by the corset of her top. “Deny us both?”
She exhaled shakily, her head dropping back against the wall. Damn him. Damn him to hell.
“It was just sex.” She tried to convince him, herself, maybe the both of them. It was hard to say and focus with such a talented mouth going to work on her bosom.
“We both know it was much more than that.” He spoke with a hint of humor, running his tongue up the middle of her cleavage. Y/N whimpered, shaking her wrists in an attempt to free herself from him. Again, she was unsuccessful. “Y/N.”
“Why can you not just leave me be?” She questioned with helplessness. “Why can’t you cast aside your feelings for me?” Her eyes were starting to water as T’Challa lowered their hands, lessening the distance between them so that their chests were almost touching. “Surely there are plenty of other women in Wakanda. Why must you like-“
“This is not a case of me liking you, sthandwa sam.” He interrupted with swiftness, his voice dripping with sincerity.
Y/N’s stomach dropped as she suddenly wished she had never gone to his room.
Or Wakanda, for that matter.
“What?” She breathed, her heartbeat going at an astronomical rate. Damnit, this sanctuary really was turning into purgatory.
The princess waited for the king to say something but instead watched as his gaze hardened with irritation.
“Stand down, boy.”
She frowned. “What are you-“
“Let her go.” Her eyes widened at the sound of Dumi’s voice. “Now.”
T’Challa growled and released her wrists, Y/N immediately deprived of his surprisingly warm touch.
“What did you just say?” It was almost rhetorical, but the menace and challenge in his voice were undeniable. “Have you forgotten who I am? Your place?”
“Dumi, stand down.” Y/N instructed as she moved between the two men, placing her hands on T’Challa’s chest.
“My place is to protect the queen.” Dumi retorted smoothly as he continued to hold his hand on his sheathed sword. “And I care not who I have to strike down to do so.” A beat. “Even if that includes the mighty Black Panther.”
At that, T’Challa ripped himself from the princess hold and grabbed Dumi, shoving him against the wall.
“T’Challa, let him go!” She pleaded, placing her hands on his bicep.
“You speak not to the Black Panther, but to the king.” T’Challa sneered. “And consider that a blessing from Bast for the politician is much more lenient than the warrior.”
“T’Challa!” Y/N yelled his name again, moving her hands to his waist, finally getting him to look at her. “Please.” She stared at him with pleading eyes, praying that she could get through to him, trying not to show her own fear.
She’d never seen this side of T’Challa.
However, she released a breath of relief when he finally let go as she moved her body in front of his. “If you ever pull a stunt like that again, you will be removed from your duties-“
Dumi’s nose flared. “He was hurting you!”
“Raise your voice with her again, and it’ll be one of the last things that you ever do,” T’Challa threatened calmly.
She shut her eyes and avoided snapping at the king. “Do I look as though I am harmed? I am fine, Dumi. Now go.” She stressed. “That’s an order.”
Dumi looked from the princess to the king, a look of abhorrence and disappointment in his face. She was prepared to speak again when her guard turned on his heel and disappeared down the hall.
As soon as he was gone, T’Challa shared, “I don’t trust him.”
“Why? Because he does his job.”
“He is too invested and not into the right things.” He shared. “His loyalty is questionable.” Before she could further protest, T’Challa continued. “Why would he send Bunme, a five-year-old, alone, to navigate a palace in the middle of the night?”
Y/N frowned. “What are you talking about?”
“Last night.” He stepped closer to her, neither moving as he placed a hand on her hip. “She told me that he told her you were in my room and sent her, by herself, to go find you.”
“He told me that she snuck away.” Y/N explained, and she had no reason to doubt him as she knew better than anyone that her daughter was one clever child. That little girl could weasel her way out of the most secure situations. “That explains how she just so happened to end up by us.”
T’Challa recognized the look of realization. “What is it?”
“I never told him that I was going to see you. I said that I was going for a walk.”
He shook his head. “You didn’t have to. He’s a man. He knew exactly where you were going and who you were going to see.”
She blushed and dropped her gaze before clearing her throat. “I will talk to him.”
“Or I could.”
“I said talk, not maim.”
“You do not believe that I can control myself?”
“That-“ she gestured down the hall. “-was control?”
“He still lives, does he not?”
“Too much, T’Challa.”
His eyes squinted ever so softly as he leaned forward, grabbing her hips and pulling her against him. His mouth dipped against her ear. “And yet you take me so well.”
She turned her head and rolled her eyes, but he could still see the faint smile on her face as she shoved him off and walked away, purposely swaying her hips in the process.
♔ ♔ ♔ ♔ ♔
Y/N was reading a book, which book, she knew not or which page, just that it had occupied her thoughts and mind for the past thirty minutes as a way to keep her from thinking about everything else.
She wanted to talk to Dumi, needed to speak with him but was in no state of mind to do so.
How could she when the king of Wakanda had practically implied that he loved her? As if things weren’t bad enough already. She just really wished she’d stayed in her room last night, except she didn’t, and now she had to deal with the consequences.
Yet…..there was a small part of her that didn’t regret what happened. Waking up with T’Challa, her daughter snuggled between them, the three all so peaceful, there was a sense of normalcy that accompanied that image. Something about that which made her feel like she could get used to it. Like she could get used to him.
Damn.
“The History of Us,” She looked up from her book to see Erik leaning against the open door of the massive palace library with his signature smug smirk. “And here I was thinking that you were tired of hearing about Wakanda.”
“Erik.” She found herself smiling. “Please.” She patted the seat next to her, watching as he sauntered over before reaching over before to give him a hug. “Welcome back.”
“Thanks.” He chuckled, eyeing her up. “I miss anything?”
She paused. “Nothing noteworthy. I attended Public Training Day.”
“Heard you did more than just attend.”
She narrowed her eyes. “If you already knew, then why’d you ask?”
He shrugged. “And miss out on an opportunity to hear about someone kicking Challa’s ass? Shit, you must not know me very well.”
She giggled softly. “Where did you go?”
His gaze visibly softened before he cleared his throat. “To go see my mom.”
“She is American?” It made sense. The way Erik dressed, his lack of an accent, his Westernized way of dressing, and the whole nine yards.
He nodded. “She’s a professor down in California, over at Stanford.” He then went on to briefly explain how his parents never married, having conceived him when his father briefly visited America and how he spent his summers in Cali with her but the rest of his time in Wakanda with N’Jobu.
“Does she ever come to visit you?”
“Now that T’Challa has opened up Wakanda, that’s the plan.” He said, leaning back into the sofa and spreading his left arm over the top. “What?”
“What do you mean, now?”
“Come on, you know we never use to allow outsiders. It was the law. Ever since the beginning of our foundation.”
“Why?” She pressed, not even hiding her shock.
“Vibranium. It’s too powerful and valuable to fall into the wrong hands.”
“And you all are so perfect and faultless compared to the rest of the world?”
Erik grinned. “We’ve gone without incident thus far.” A beat. “But it makes no difference now, once T’Challa came back from Oxford and took the throne from my pops-“
“Your father used to be king?” Her eyed widened. This was all such surprising news to her and a much-needed distraction.
He nodded. “After T’Chaka was killed, T’Challa was too young and, obviously so was I, so the mantle fell to the next in line which was my father.”
She followed the chain of thought. “So technically, you could have been king too?”
“If I challenged him.”
“But you didn’t.”
“Politics isn’t really my thing.”
“Perhaps you just don’t think you could best your cousin in battle,” she teased with a small smile.
Erik chuckled. “You’d lose that bet, baby girl. On any given day.”
She remained quiet, allowing everything she’d just learned to settle in before speaking again. “So, once T’Challa became king, he reversed the law?”
He nodded. “One of his first acts.” His eyes fell on her. “Maybe now I know why.”
She picked up on his indication. “Oh, please.”
“What?” He shrugged. “If I was him, I’d make it so the woman that I love and my daughter could come to visit as they so pleased.”
Y/N’s heart stopped and her mouth dried as she snapped her head in his direction. “What did you just say?”
“Relax, your little secret is safe with me and pops-“
She tried not to show her panic at the mentioning of the fact that not only did he know the truth, but N’Jobu did too. “I don’t know what-“
“I’m sure you don’t,” he winked, standing up and stretching. “A little advice though? Tell him. He deserves to know the truth, Y/N.”
And with that, Erik left the stunned Princess of Niganda with many, many thoughts and situations to ponder.
♔ ♔ ♔ ♔ ♔
T’Challa walked into his room later that evening and stopped in the doorway.
“Hi, kitty!”
He couldn’t even stop his smile despite his confusion. “Hello, sam isipho.”
The energetic little princess was settled in the middle of his bed with a vibranium tablet, notebooks and other school supplies surrounding her. Of course, her doll was with her too.
He started to ask how she’d gained access to one of the arguably most secure rooms in the place but decided against it. It honestly didn’t matter. He doubted few could deny the child anything, period.
“Are you busy?” She tilted her head to the side and pouted slightly.
“For you? Never.”
That earned him a giggle. “Can you help me with my homework? I can’t find Shuri and bad kitty is being a meany head.”
“Bad kitty?”
She shook her head. “Erik.”
T’Challa mentally rolled his eyes and made a notation to ask Erik to politely return the Jaguar Habit back to the lab asap.
“Of course, I will help you.” He kindly agreed and motioned for her to follow him over to the sofa on the other side of his spacious bedroom. He watched with amusement as the child climbed off his bed with her dolly, tablet, and notebook, skedaddling over to join him on the expensive piece of furniture.
“It’s just the math that I don’t know.” She started to explain taking the king by surprise as she nonchalantly lifted one leg onto the sofa and then crawled over into his lap, making herself comfortable as she started to point out her area of difficulty. “Stay right there.” She wagged a finger to her doll that was sitting up beside them, earning a small chuckle from the Black Panther.
“Ah, I see what the problem is.” He started before going into a concise and lucid explanation for the child, watching in astonishment as she picked up on the concept in less than five minutes. “Brilliant.”
“That’s what my teacher said!” Bunme beamed while looking up and over at him. “She said I’m really...um.....umm...”
“Bright?” He suggested.
“Yeah!” She pointed with excitement before her smile dropped. “That’s good, right?”
“It is excellent.” He complimented. “You are a very special little girl, Bunme.” She retained her smile before it dropped again. “What’s wrong, sam isipho?”
“Can I ask you a question?”
“Of course. You can ask me anything.”
“Well.” He watched her twiddle her fingers. “You have a mommy and a sister and other family....where’s your daddy?”
He froze, not expecting the question but handled it as best he could. “Bunme, do you remember when you told me that bad people killed your father?” She shook her head. “Well, when I was a little boy, not much older than you, a bad man killed my father.”
Bunme gasped in shock and once again surprised the king as she leaned into him, placing her tiny arms around his body in an attempts to give him a hug. “Stupid, meany head, bad man.”
His lips lifted into a small and sad smile as his hand went to softly caress the back of her head. “Indeed.”
She lifted her head to look at him. “Do you remember him, kitty?”
He looked down at her. “A little. My memories are few.”
“I never met my father.” She frowned with sadness, looking down, around, and then up at him. “Do you think he would have liked me?”
He answered without hesitation. “He would have loved you, Bunme.”
She grinned with pure appreciation. “Kitty, when mommy and I go back....is it....is it okay if I come back and visit you?” Again, her smile faltered slightly. “I like it here, and...I don’t want you to forget me.”
T’Challa’s heart sank not only from the child’s statement but just from the mere thought of them leaving.
He didn’t want them to go.
Not now.
Not soon.
Not at all.
“Here.” He put his hands around his neck and pulled a necklace out of his collar. “I want you to have this.” She watched in awe as he removed the necklace with a black vibranium pendant on the end in the shape of a Panther on it and placed it around her neck.
“It’s a kitty!” She exclaimed with wide eyes of excitement while observing it.
“It is.” He confirmed, carefully watching her. “Passed down in my family for generations. My own father gave it to me, a gift from his father to him and so forth, and now….I am giving it to you.”
She looked slightly confused as she squinted one eye. “Isn’t it special to you?”
“It is, but so are you.” He answered, watching as her smile started to reappear. “And now you know that I shall never and could never forget you, Bunme.”
At that, the little girl lost it. She got on her knees while still in his lap and attacked him with a better version of her previous hug, wrapping her arms around him as she whispered in his ear. “I think your daddy would think you’re a really good kitty.”
T’Challa quieted for a moment as the little girl’s words deeply resonated with him even if she didn’t realize exactly what she was saying. Being a good ‘kitty’ aka king, Black Panther, making his father proud.....that was all he wanted for the late King T’Chaka’s legacy. Somehow, hearing it out of her mouth solidified his latent fears.
He closed his eyes and lightly kissed her temple. “Thank you, sam isipho.”
“I think he’d also want us to get ice cream.” She whispered while his lips were still pressed against her temple.
The king laughed loudly. “Is that so?” She nodded fervently. “Well then....” Bunme started laughing loudly as T’Challa stood up with her in his arms, switching her so that she was on his hip, placing a kiss to her cheek as she held onto his neck. “Ice cream we shall get.”
“Yay!” She cheered as the two left the room, Bunme not even remembering the infamous doll that still sat on the sofa.
Welp. So Erik knows? And N’Jobu?
And Dumi.
Imma just tell you right now.
T’Challa don’t like his ass. The feeling is mutual though so....
Wonder if anyone else does....hmmm.
I decided to pull from the comics in terms of backstory because I felt it goes better with this storyline.
Also, question.
I’ve been receiving comments and questions that my stories and characters are too loaded and intricate to be “Y/N” aka reader stories. Do you all agree? Should this be switched over to a T’Challa x Main Character story? Literally, nothing would change except “Y/N” would have a name, and I’d provide a picture of how I imagine her looking. lol
Because we already have a picture of our child Bun Bun.
Or we can totally leave things as they are. I’m perfectly content with either option. Truly.
Let me know!
#black panther imagine#black panther fanfiction#t'challa x reader#T'Challa Udaku#black panther#Erik Killmonger#t'challa#fluff galore#space between#t'challa x storm#t'challa x mutant!reader#Bun Bun Wednesday
357 notes
·
View notes
Text
Rules of Infatuation
by longbeachtrekstar, 2005
The women of the house celebrate an old Ferengi tradition.
Words: 3253, Chapters: 1/1, Language: English
Rating: NC-17
Warnings: none listed
Characters: Ishka, Kira Nerys, Jadzia Dax, Leeta, Deanna Troi, Lwaxana Troi
Relationships: Kira/Jadzia Dax, Kira/Jadzia Dax/Leeta/Deanna Troi/Lwaxana/Ishka
Reader suggested tags (what are these?): crossover - Star Trek: The Next Generation, Femme Fuh-Q Fest (round 19)
links (link broken? report it and try the archive.org alternative):
trekiverse
archive.org - option 1 [Archivist’s note: NSFW image at top of page.] / option 2 / option 3 [Archivist’s note: NSFW image at top of page.]
#year2005#citrusfic#ishkafic#majorkira#jdax#leetafic#lwaxanafic#kirajdax#kiramisc#jdaxleeta#jdaxmisc#leetamisc#lwaxanamisc#ishkamisc#ishkalwaxanafic#jdaxishkalwaxana#kiraleetafic#2kto5k#crossover: ST TNG
0 notes
Text
For anyone in New York State: senate bill 3253-A gives you the right to record police, peacekeepers, or security officers as they conduct law enforcement activity, as well as the right to retain that recording and the device it was recorded on. It prohibits police from attempting to stop you from recording them, or harassing you for doing so. If they do, you can bring them to court, and the court may cover your legal fees.
The bill is less than 3 pages. Read it if you can. Know your rights.
PSA to my white friends and followers: In the wake of a phenomenally important guilty verdict in the Derek Chauvin Trial, I’d like to remind you all that the fallout of this case will likely mean more police violence against our Black friends and neighbors, not less. Looking at the statistics in the weeks leading up to this verdict shows that this is already the case. Police in this country are angry that society is beginning to hold them accountable for their abusive actions, and they are looking for revenge. So if you see a cop interacting with a BIPOC, DO NOT walk away. Video record if you can (and as long as it doesn’t further jeopardize the safety of the BIPOC involved), but absolutely do not walk away. It is critical that we do our part and look out for people, and make cops think twice about abusing their powers of authority and near-immunity to murder citizens.
63K notes
·
View notes
Photo

We are supplier to the rock drill equipments (Underground and Surface) - DRIFTERS ALTERNATIVE SPARE PARTS (COP Series of Atlas Copco) (HL Series of Sandvik) (HC Series of Montabert) (HD Series of Furukawa) - JUMBO MACHINE ALTERNATIVE SPARE PARTS (BOOMER Series of Atlas Copco) (DD Series of Sandvik) - ROCKDRILL MACHINE ALTERNATIVE SPARE PARTS (ATLAS COPCO) (SANDVIK-TAMROCK) MONTABERT) (FURUKAWA) (INGERSOLLRAND) For your orders: WhatsApp Number: +90 532 137 49 39 E-Mail: [email protected] / [email protected] Osman ERCİYAS General Manager please follow our page and contact if you need something ([email protected]) (+905321374939 ) #hydraulicrockdrill #hydraulicrockdrillspareparts #hydraulicdrifter #hydraulicdrifterspareparts #atlascopcorockdrill #atlascopcorockdrills #atlascopcorockdrillspareparts #epirocrockdrills #epirocrockdrillingtools #atlascopcodrifter #atlascopcodrifterspareparts #epirocdrifter #epirocdrifterspareparts #atlascopco #epiroc #mining #drifters #drifterspareparts #atlasroc #atlasrocd7 #atlasd7 #cqbinairfilter #kabinfiltresi #3222325376 #3222 3253 76 #3222-3253-76 #efsgrup #www.efsgrup.com.tr (Ankara Ostim) https://www.instagram.com/p/CXdH3TKsye-/?utm_medium=tumblr
#hydraulicrockdrill#hydraulicrockdrillspareparts#hydraulicdrifter#hydraulicdrifterspareparts#atlascopcorockdrill#atlascopcorockdrills#atlascopcorockdrillspareparts#epirocrockdrills#epirocrockdrillingtools#atlascopcodrifter#atlascopcodrifterspareparts#epirocdrifter#epirocdrifterspareparts#atlascopco#epiroc#mining#drifters#drifterspareparts#atlasroc#atlasrocd7#atlasd7#cqbinairfilter#kabinfiltresi#3222325376#3222#efsgrup#www
0 notes
Text
HealthWatch Review
I was scouring the net for a quality fitness tracker watch when I came across an advert of this watch. I must say that I was a little skeptical about its functionality, but when I received it and started using it, I could see why many health and fitness swear by it. I found the heart rate monitor, the calorie calculator, and the blood pressure monitor most helpful.

The real-time information the watch could give me during my workout sessions turned out to be very helpful in the long run as I used to make gradual developments towards better health. In summary, the watch works just like the manufacturer promises. It the functions listed by the manufacturer perform just right. If you like working out or doing sport, you will definitely like this product.
Benefits of Using HeathWatch
The smartwatch comes with a raft of benefits which include:
It gives you analyzed data on how various body systems are functioning in real-time
You can use the information it gives you to track your fitness activities and improve your health
It is compatible with Android and iOS devices so you can receive incoming calls and messages notifications
You can take photos with it
It can monitor your sleep so you know if you are sleeping well
It keeps track of your activity during the day
With its multi-sport mode, you can monitor a variety of sports activities such as swimming, football, basketball, cycling, et cetera
It is easy to use
HealthWatch Key Features
Heart Rate Monitor; Measures your heart rate and gives you data in real-time
Blood Oxygen Level and Blood Pressure Monitor
Calorie Calculator; Tells you how many calories you have burned in kilo-calories
Multi-Sport Mode; Monitors various sports activities like cycling, soccer, and swimming
Sleep Monitor
Social Network Notifications
Compatible with Android and iOS, which allows call and message notifications
http://www.lenas-kochbuch.de/phpBB2/viewtopic.php?p=799407#799407
http://www.cruzroja.es/creforumvolint_en/user/profile/138052.page
http://www.mallora-immobilien-direkt.de/forum/memberlist.php?lang=es&mode=viewprofile&u=30629&sid=b69cafa8c8e1456feced183e70740241
http://www.golfgtiforum.nl/portal/viewtopic.php?f=32&t=12319&p=170452&sid=f0f4471a4a39b69e924a74f65da04196#p170452
http://www.shoesession.com/forum/memberlist.php?mode=viewprofile&u=108189
http://melanz.phorum.pl/memberlist.php?mode=viewprofile&u=122075
http://smolmama.com/forum/memberlist.php?mode=viewprofile&u=19770
http://www.asingularcreation.com/Forums/viewtopic.php?f=33&t=13337&p=69004#p69004
http://thenightshiftgaming.com/forums/memberlist.php?mode=viewprofile&u=732026
http://crowdfundingforum.com/member.php/52264-natrajan
http://peepsglasscleaner.canariblogs.com/peeps-eyeglass-cleaner-review-14517181
https://www.codeleakers.com/showthread.php?93650-The-Photostick-Mobile-Review&p=681926#post681926
http://www.escalade-alsace.com/forum/profile.php?mode=viewprofile&u=11264&sid=585d1c83bc657b7050cfa5e608f79bbe
http://www.freecpapadvice.com/forum/viewtopic.php?f=10&t=6260
http://www.weisheqi.com/home.php?mod=space&uid=1851173
http://forum.meogames.com/home.php?mod=space&uid=2559504
http://www.pcmaster.gr/forum/viewtopic.php?f=7&t=123755
http://forum.echo.or.id/forum/memberlist.php?mode=viewprofile&u=63019&sid=76cd17b8f5cfe1da5ddc9b264faa18e6
http://www.ipnvrj.com.br/forum/profile.php?mode=viewprofile&u=711767
https://forum.dchublist.org/viewtopic.php?f=3&t=24&p=1040#p1040
https://healthzaa.com/sites/done21.com/
https://www.travelaz.net/sites/done21.com/
https://advancedsitestats.com/done21.com/
https://www.healthgolds.com/sites/done21.com/
https://usfitnessfinder.com/site-fitness/done21.com
http://www.letsgoo.de/index.php?site=profile&id=371
https://golden-forum.com/memberlist.php?mode=viewprofile&u=105845
https://www.vgcheat.com/forum/members/ankur11/
https://www.healthlifes.info/sites/done21.com/
http://quanticode.com/forum/phpBB3/memberlist.php?mode=viewprofile&u=13982&sid=416df8487571d308b4456b14dcab14dc
http://forum.kpn-interactive.com/viewtopic.php?f=3&t=66110&p=79759#p79759
https://www.softwarezz.info/done21.com/
https://www.forum.doripesco.ro/forum/thephotostick-review
http://www.consolegames.ro/forum/members/ankur11/
http://forum.computer-technology.co.uk/viewtopic.php?f=33&t=6771&p=16016#p16016
http://empyrethegame.com/forum/memberlist.php?mode=viewprofile&u=52987&sid=3932a76d403286369f048efd0eb81e8b
http://smolmama.com/forum/posting.php?mode=reply&f=398&t=28543
https://www.dizzysupport.org/community/viewtopic.php?f=2&t=3253&p=3408#p3408
https://forum.supraboats.com/member.php?41378-ankur11
http://azs-bialystok.pl/forum/member78840.html
https://forum.openbadania.pl/memberlist.php?mode=viewprofile&u=54161
https://forum.racing.by/memberlist.php?mode=viewprofile&u=17328&sid=8f7fa6648e9488d2798f9fbd6d6be394
https://tgstation13.org/phpBB/memberlist.php?mode=viewprofile&u=61281
http://forum.ppr.pl/profile.php?mode=viewprofile&u=421106
http://www.dislivelli.eu/forum/viewtopic.php?f=6&t=1085&p=2048#p2048
http://www.satpasaulis.lt/memberlist.php?mode=viewprofile&u=22742
https://www.jeepstrokers.com/forum/memberlist.php?mode=viewprofile&u=8369
http://forum.mymp3board.com/profile.php?mode=viewprofile&u=1311
https://carriefans.com/forums/showthread.php?t=161149&p=4812399&posted=1#post4812399
https://filesharingtalk.com/members/459087-ankur11
https://www.scifi-forum.de/member/43772-ankur11
https://forum.benchmark.rs/members/ankur11.226734/
https://www.vwvortex.com/members/ankur11.3817018/
http://www.aytoloja.org/jforum/user/profile/131018.page
https://www.ukmix.org/forum/ukmix/happy-20th-birthday-ukmix-forums/happy-20th-birthday-ukmix-forums-aa/10552050-happy-20th-birthday-ukmix-forums/page2#post10598566
https://www.tidalfish.com/members/ankur11.207584/
https://surf-forum.com/user/9765-ankur11/
https://www.rcuniverse.com/forum/members/ankur11.html
https://www.airgun101forum.com/index.php/photostick
https://www.planetcalypsoforum.com/forum/index.php?members/ankur11.66512/
https://www.done21.com/peeps-glass-cleaner-review/
https://www.drone-forum.com/forum/memberlist.php?mode=viewprofile&u=17882
https://www.italiarec.com/forum/members/1692-ankur11
https://www.pedelecforum.de/forum/index.php?members/ankur11.80281/
https://www.adisc.org/forum/members/ankur11.56392/
https://hopeinenomena.fi/viewtopic.php?f=44&t=282183&p=2106033#p2106033
http://masa.asn.au/phpBB3/posting.php?mode=reply&f=110&t=269891
http://forum.programosy.pl/viewtopic.php?f=3&t=150645&p=1048912#p1048912
https://www.camfaith.org/cforum/posting.php?mode=reply&f=6&t=14
http://forum.psyradio.com.ua/showthread.php?p=316867#post316867
https://forum.singaporeexpats.com/memberlist.php?mode=viewprofile&u=283401
http://bbs.co.99.com/member.php?u=465062
http://www.deepspacenyc.com//modules.php?name=Your_Account&op=userinfo&username=ankur11
http://qa.rmutto.ac.th/phpBB3/viewtopic.php?f=5&t=1733742&p=2672058#p2672058
http://www.rippedmass.org/forums/anabolic-discussion-forum/13569-sponsor-get-your-needles-syringes-here-305.html#post848329
http://silber-gold-forum.de/Forum/memberlist.php?mode=viewprofile&u=7334&sid=1550365c6f125ed925015feed9298d03
http://choxinh.com/member.php/846400-ankur11
http://ciphertalks.com/viewtopic.php?f=8&t=712342&p=1537263#p1537263
http://49.231.238.163/board/posting.php?mode=reply&f=3&t=1601968#preview
http://unraveled.net/phpbb/posting.php?mode=reply&f=6&t=2076890
https://www.sitelinks.info/done21.com/
https://healthzaa.com/sites/done21.com/
https://dashburst.com/ankur11
https://dashburst.com/ankur11/boards/health
https://ecouponscodes.com/site-coupon/done21.com
https://www.healthgolds.com/sites/done21.com/
https://usfitnessfinder.com/site-fitness/done21.com
https://www.travelaz.net/sites/done21.com/
https://forums.suck-o.com/viewtopic.php?f=59&t=12172&p=87894#p87894
https://www.hojko.com/post2377393.html#p2377393
http://crpsc.org.br/forum/viewtopic.php?f=3&t=280632&p=831216#p831216
http://forum.winnerinter.co.id/forum_21/blog-74933-2345.html
http://conceptdistributing.com/UTVinCanada/viewtopic.php?f=13&t=8496&sid=4219c6ad693655db7d02f45b8e09fbcc
http://forum.kpn-interactive.com/viewtopic.php?f=3&t=68579
http://www.rippedmass.org/forums/anabolic-discussion-forum/205159-bzhyxw-rtmnak-kakiec-rhvkpq.html#post850074
https://www.lawschool.life/forums/memberlist.php?mode=viewprofile&u=44399
http://imagination.lt/the-photostick-mobile-review-t70467.html
http://my-mallorca-property.com/forum/viewtopic.php?lang=en&f=15&t=247813&start=0&sid=73286097506c1186e7b0db3315c9d508
http://forum.mbclub.lv/posting.php?mode=reply&f=89&t=12496
http://www.asingularcreation.com/Forums/viewtopic.php?f=33&t=13516
http://forum.audiosila.com/member.php?u=8411
http://www.volksforum.com/forum/showthread.php?p=1673119#post1673119
http://www.magrace.ru/forum/viewtopic.php?p=1540424#1540424
http://cncportal.ru/forum/profile.php?mode=viewprofile&u=402791
http://bustalk.info/forum/viewtopic.php?p=42877#42877
https://forum.dchublist.org/viewtopic.php?f=3&t=523
https://forum.mt5.com/member.php?1346095-ankur11
https://3dprintboard.com/showthread.php?49391-Health-Watch-Review&p=152946#post152946
http://www.flyingfish.nl/forum/viewtopic.php?p=2852699#2852699
http://www.rapbattles.com/forum/showthread.php?499846-1-2-PUNCH-SIGN-UPS&p=8943499#post8943499
http://forum.9dots.de/profile.php?mode=viewprofile&u=14848
http://corsica.forhikers.com/forum/p/49574
http://www.chemport.ru/forum/viewtopic.php?f=55&t=134391
https://ancestralelements.com/community/ancestral-elements-podcast-forum/photostick-mobile-review/
https://forum.wdwnorth.com/posting.php?mode=reply&f=4&t=157856
https://exposingtheothers.com/forum/member.php?action=profile&uid=3896
https://coderbd.com/forum/spring-boot/healthwatch-review/
https://bowl.hu/forum/nfl-altalanos-temak/sport-tv-hori
http://foro.audiomusica.com/memberlist.php?mode=viewprofile&u=183249
https://forum.openbadania.pl/memberlist.php?mode=viewprofile&u=63537
https://www.lawschool.life/forums/memberlist.php?mode=viewprofile&u=45684
http://www.consolegames.ro/forum/members/ankur12/
http://www.mallora-immobilien-direkt.de/forum/memberlist.php?lang=es&mode=viewprofile&u=34156&sid=68a9d244a29d5b99ffd670561b4fda51
http://www.golfgtiforum.nl/portal/memberlist.php?mode=viewprofile&u=7624&sid=b7758d928660bf5f323cb1e7512c0c20
http://forum.topclimat.ru/profile.php?mode=viewprofile&u=210376
http://forum.rockguru.ee/profile.php?mode=viewprofile&u=349894
https://www.domaininfofree.com/domain-traffic/done21.com
http://gamerspark.vforums.co.uk/action/view_profile/user/ankur11
https://www.extelicast.com/ankur11
https://www.ethicalhacker.net/members/ankur11/profile/
http://welcome2solutions.com/forum/profile.aspx?ID=143652
https://health-medical.info/site/done21.com/
https://www.tourbr.com/story/tikitunes-review-bluetooth-speakers-the-best-in-class/
https://www.knowpia.com/s/blog_c878a1899eb141c1
http://forum.kpn-interactive.com/viewtopic.php?f=3&t=75549&p=98976#p98976
https://www.zombiepumpkins.com/forum/memberlist.php?mode=viewprofile&u=65527
http://empyrethegame.com/forum/memberlist.php?mode=viewprofile&u=74387&sid=522cdb120d404c068129c0004dfd652c
http://www.leatherneck.com/forums/member.php?128100-ankur11
http://chat-place.org/forum/viewtopic.php?f=30&t=129234&sid=36706458f0d283f4f2624f62d4a23a06
0 notes
Photo

New Post has been published on https://factory.sweb-demo.info/product/moc-12653-battlestar-galactica-ucs-cylon-raider-ucs
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
After my UCS Colonial Viper MkII, right here is the UCS Cylon Raider, impressed from the reboot sequence! Built on the similar scale because the Viper, will probably be the proper match. Ligthing results will be simply added, and can give your mannequin a remaining agressive contact.For this mannequin once more, you should purchase the constructing directions as a top quality 326 pages pdf, which incorporates the ready-to-print UCS sticker, in addition to separated half lists for the show stand and for the Raider itself. The half lists are additionally supplied as an XML information. Just head over to BrickVault web site! So Say We All!
Comments 5
Inventory 3253
Buy Parts ?
Building Instructions
Photos 12
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by acroporabonsai PRO
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by texgordon PRO
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by texgordon PRO
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by jackalope
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by jackalope
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by jackalope
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by jackalope
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by jackalope
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by jackalope
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by jackalope
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by jackalope
MOC-12653 Battlestar Galactica UCS Cylon Raider UCS
by jackalope
0 notes
Link
The advantage of gambling on the Dominoqq website is that it provides you the access of the various odds of bookie. In case in the event you carry out your study before betting and bet prudently, it can also raise your possibilities of winning a bet. The way you are able to register with Dominoqq website-it is extremely comparable towards the way you register with any other online poker. Firstly access the page of registration using the help of Google Translate to ensure that you are able to comprehend the instructions and follow them cautiously.
0 notes